 IB Docs (2) Team
IB Docs (2) Team

Amir et al (2015)
 This study can be used to support the use of psychological treatments for people with OCD. It may also be helpful in evaluating biological treatments, e.g. comparing the efficacy of drug treatments with ERP and/or CBM.
This study can be used to support the use of psychological treatments for people with OCD. It may also be helpful in evaluating biological treatments, e.g. comparing the efficacy of drug treatments with ERP and/or CBM.
Despite strong evidence to support the efficacy of Exposure Response Prevention (ERP) therapy in reducing OCD symptoms, it requires a highly trained therapist, making it an expensive and inaccessible option for many people. Making ERP more accessible is therefore a priority. One possibility is self-directed therapy (sERP). Here the client works through a program designed by a trained therapist, but it is completed independently, via computer or mobile phone. Unfortunately, this mode of delivery is too challenging for some people; the exposure element is hard, especially in the absence of a reassuring therapist to support and motivate them. This can lead to non-compliance and failure to complete the program. Greist et al. (2002) found a dropout rate of a massive 50% for sERP. For this reason, psychologists are seeking ways of improving the therapy.
This study examines the effect of combining ERP and Cognitive Bias Modification (CBM), a technique previously shown to be helpful in encouraging compliance. For example, Najmi and Amir (2010) found that people with contamination-related OCD who completed a program targeting attention bias (CBM-A) completed more steps in their ERP hierarchy than those who did not complete the CBM-A program.
The aim of the current study was to test the efficacy of a self-directed treatment program for OCD integrating sERP with CBM and also to explore whether different types of CBM are more effective than others.
22 people (14 male and 8 female) who met the OCD diagnostic criteria participated in a seven-week treatment program. They were each assessed using the Y-BOCS interview to assess the severity of their symptoms on a scale of 0 - 40 and completed a battery of tests, including measures of interpretation and attention bias. These measures were all taken again at the end of the study to compare scores before and after treatment. In other words, the study used a pre-test/post-test design.
The ERP therapist worked together with the clients to create a fear hierarchy by gathering photographs of objects and situations that reflected thoughts and situations associated with their symptoms. The clinician conducted a practice ERP training session with the participants. In addition to the ERP exercises using their personal hierarchies, they also participated in different CBM tasks each week. Tasks were counterbalanced so that everyone completed all five tasks but the order was varied to eliminate order effects and increase internal validity. The tasks included interpretation bias modification, attention bias modification, attention control, working memory training, and a control task.
Interpretation bias task: A word representing either a threat interpretation (e.g., “dog-poop”) or a benign interpretation (e.g., “twig”) appears in the center of the computer screen for 500 ms. Next, an ambiguous sentence (e.g., “I stepped on something brown”) appears and on the screen and the computer prompts participants to press a key if they thought the word and sentence were related (agree) or to press another key if they thought the word and sentence were not related (disagree).
Attention control task: During each trial a fixation sign (either +,−, or 0) appears for 500 ms, followed by a negative, neutral, or positive word that appears in either the left or right side of the screen for 500 ms. An arrow appears in either the same or opposite location as the word for 16 – 500ms. Participants are instructed to respond with a right or left mouse click indicating the direction of the arrow (pointing up or down).
Over the next five weeks, the participants completed sERP + CBM training sessions both at home and in the clinic, where they were observed by a research assistant. They were told that access to the clinician was for emergencies only and the research assistant used standardized instructions at all times. In addition, they completed self-reported measures of their symptoms.
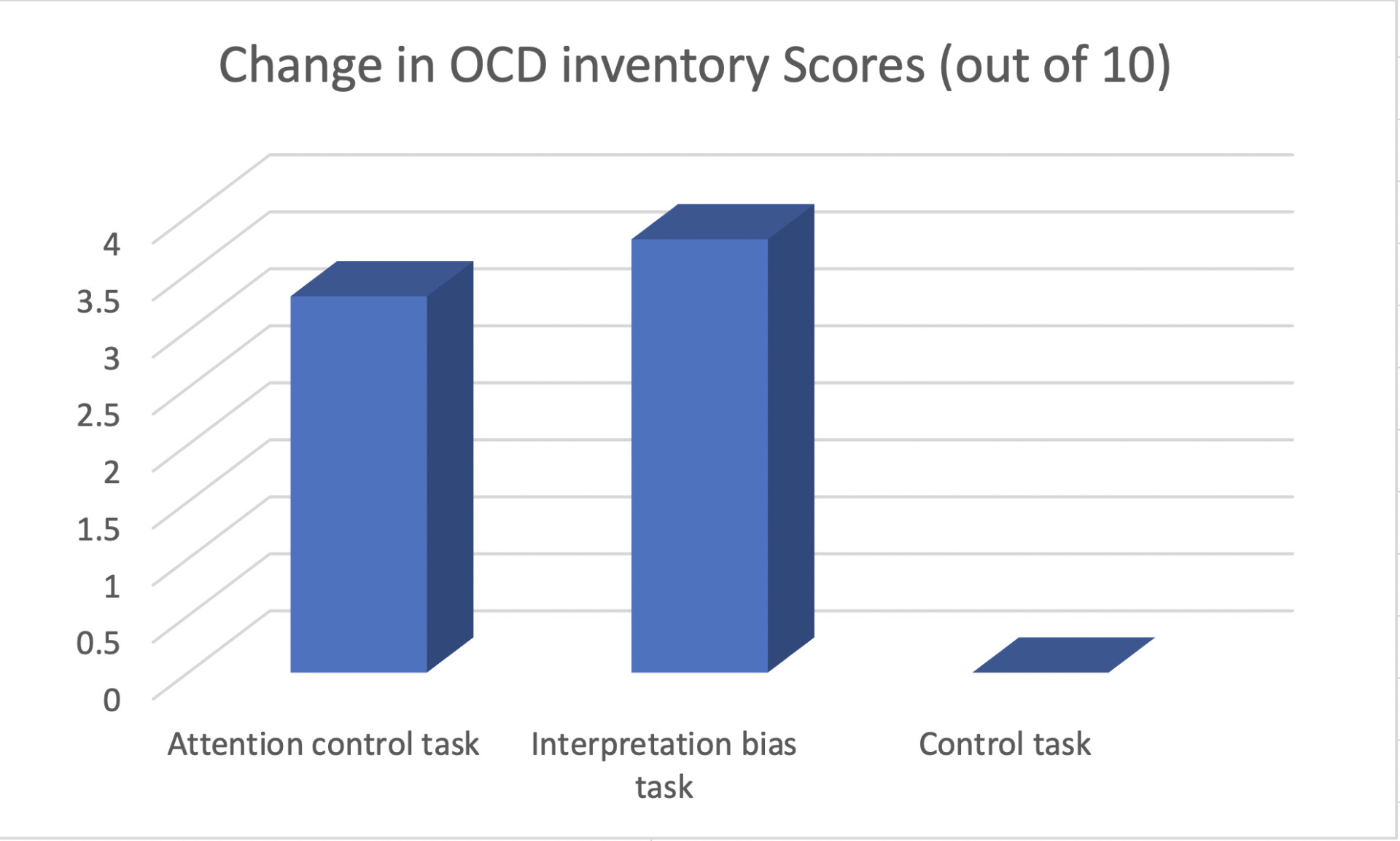 Of the four CBM tasks, only two were significant - the interpretation bias modification and attention control tasks. The control condition showed no improvement.
Of the four CBM tasks, only two were significant - the interpretation bias modification and attention control tasks. The control condition showed no improvement.
73% of the sample (16/22) completed the course. All completers showed a significant reduction in their YBOCS scores following treatment, from an average of 29/40 to 16.5/40, (p<0.001). 44% were identified as fully recovered. These very positive outcomes were also maintained in a four-month follow-up where the average YBOCs was 15/40.
The study used a pre-test/post-test design - in other words, a repeated measures design - which reduces the effects of participant variability.
Despite the therapy being self-conducted, the sessions were conducted in the presence of a research assistant so that they could be sure that the tasks were completed as expected, thus enhancing internal validity. However, this may have decreased ecological validity and increased compliance as participants may have felt more motivated to carry out the exercises, as they were doing it as part of a research study in front of a psychologist. Had the participants completed the sERP alone in their own homes, the results may have been different.
The study used self-report measures to assess the efficacy of the different augmentation strategies and participants may have given socially desirable responses, i.e. saying that their symptoms were improved more than they actually were. This said the Y-BOCS was used pre and post-intervention and this is a clinician-based assessment, based on a semi-structured interview, providing a slightly more objective view.
The sample size was relatively small reducing the power of the statistical tests. Furthermore, the sample was predominantly white caucasian (15/22). The remainder were primarily Hispanic, with only two identifying as Native American and Other. As with many studies in the field of mental health, people from ethnic minority groups are under-represented, meaning one cannot be sure whether these therapies would be effective in treating people from differing cultural backgrounds.
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn