 IB Docs (2) Team
IB Docs (2) Team

Emotion and decision making
 The Dual Processing Model of thinking and decision making suggests that we have two distinct modes of thinking: an intuitive, fast mode of thinking (System 1) and a slower, conscious, and rational mode of thinking (System 2). However, this model does not directly address the role of emotion in thinking and decision-making.
The Dual Processing Model of thinking and decision making suggests that we have two distinct modes of thinking: an intuitive, fast mode of thinking (System 1) and a slower, conscious, and rational mode of thinking (System 2). However, this model does not directly address the role of emotion in thinking and decision-making.
Emotion is an important factor in decision making, although most models do not address exactly how and why emotion might influence the way we think and the decisions we make. Many researchers believe that an increase in emotion will increase our dependence on System 1 as cognitive load is increased, making cognitive processing by System 2 difficult.
Most people would probably say that their decision-making is impaired by emotion; that we think more clearly and make more logical decisions when our thinking is free of strong emotions. However, recent neurobiological research has indicated that emotion may be essential to good decision-making.
The somatic marker hypothesis suggests that good decision-making depends on an ability to access appropriate emotional information linked to the situation in which the decision is being made.
The Somatic Marker Hypothesis (Damasio, 1994)
Neurologist Antonio Damasio noticed that some of the brain-damaged patients he was working with consistently made poor decisions, often doing things that were likely to negatively impact their welfare. This was even true when they had made the ‘bad’ decision before and suffered the consequences. Demasion's Somatic Marker Hypothesis argues that emotional processes guide decision-making.
Damasio realized  all of these patients had suffered bilateral damage (damage in both hemispheres of the brain) in the ventromedial prefrontal cortex (vmPFC).
all of these patients had suffered bilateral damage (damage in both hemispheres of the brain) in the ventromedial prefrontal cortex (vmPFC).
These patients found it hard to plan ahead and would repeatedly make the same ‘bad’ decisions which caused them to lose money, friends, or status. Most mysteriously, when their decision-making was tested in a lab environment there did not seem to be any problem; their intellect and memory capacity seemed unaffected by the damage to their brains.
Damasio began to wonder if damage to the vmPFC somehow caused patients to lose a connection between emotional information and their decision-making. The vmPFC seems to be involved in somatic markers of emotions associated with thoughts and memories. Somatic markers are feelings in the body that are associated with emotions, such as the association of rapid heartbeat with anxiety or of nausea with disgust. Domasio wondered what would happen if this layer of information was removed when we try to decide what to do in a difficult situation.
ATL: Communication
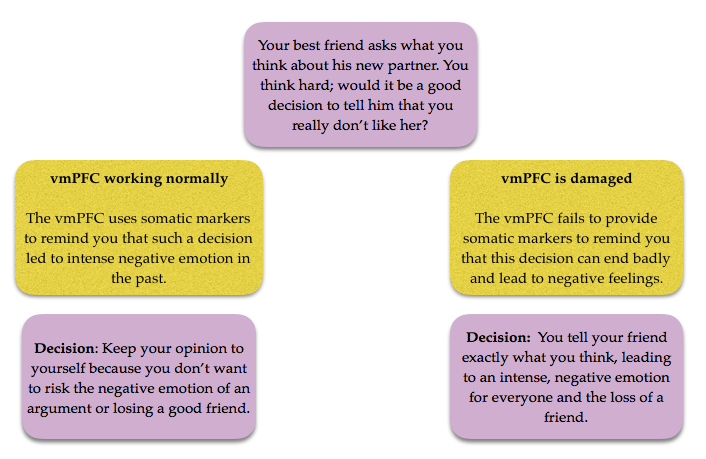
The somatic marker hypothesis can perhaps be best understood with the diagram below.
Questions
1. This diagram does not explain what the exact somatic markers are that the vmPFC would use to make this decision. What do you think they might be?
2. Create your own version of a diagram to explain the Somatic Marker Hypothesis with regard to one of the following decisions:
A. You have already had a lot to drink. Someone offers you "one more."
B. You are late coming home from a party; someone you meet at the party tells you "let's cut through this dark alley!"
1. This diagram does not explain what the exact somatic markers are that the vmPFC would use to make this decision. What do you think they might be?
Somatic markers are feelings in the body that are associated with emotions, such as the association of rapid heartbeat with anxiety or of nausea with disgust. In the past, telling someone that you did not like their new choice of partner may have resulted in the person being very angry with you. This would lead to feelings of high stress, despair, or even fear based on losing that person's friendship. That high state of anxiety and the physiological state that accompanies it would be the somatic marker.
2. Create your own version of a diagram to explain the Somatic Marker Hypothesis with regard to one of the following decisions:
A. You have already had a lot to drink. Someone offers you "one more."
There is more than one way to approach this. If having "one more drink" ended up with a terrible hang-over (pain), being sick (disgust), having a major fight with someone (disappointment), or getting robbed (fear) - these feelings should then prompt one not to have that "one last drink." However, alcohol has an effect on our ability to process that information, so it would not be a surprise that one makes a poor decision if they have already had a lot to drink.
B. You are late coming home from a party; someone you meet at the party tells you "let's cut through this dark alley!"
The somatic marker here is most likely fear - either from past experience or worry about what could happen. Sometimes when we are in a rush - e.g. trying to get home as soon as possible because you are already past your curfew - means that we do not attend to somatic markers and make poor choices.
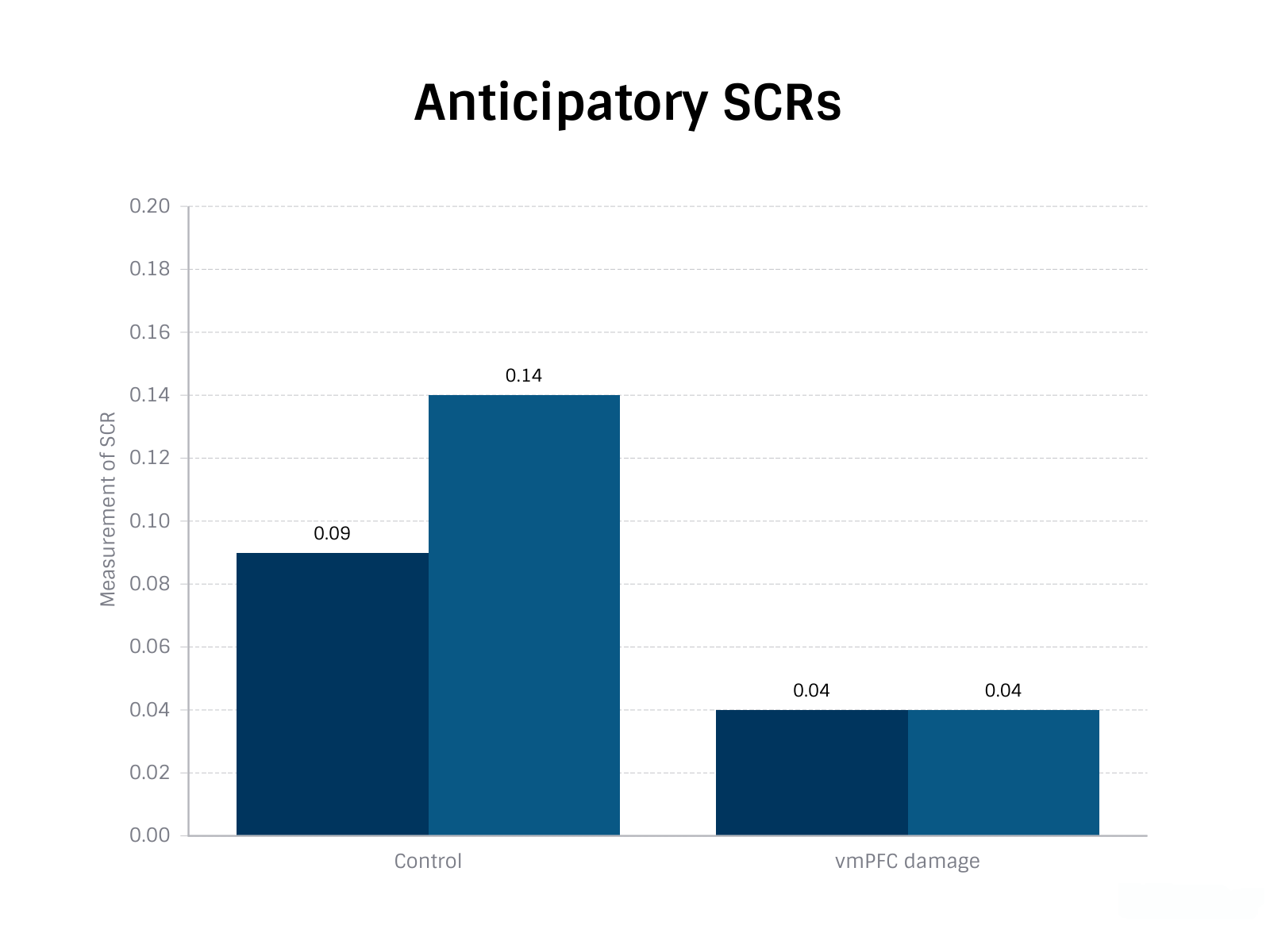
Bechara et al (1999) developed a game known as the Iowa Gambling Task to test the Somatic Marker Hypothesis. The aim of the study was to determine the role of damage to the vmPFC on decision-making. In this game, participants saw four decks of cards on a computer screen. The decks were labeled A, B, C, and D at the top end of each deck. Using a mouse, the participant could click on a card on any of the four decks. Every time the participant chose one of the decks, the face of the card appeared on top of the deck and a message was displayed on the screen indicating the amount of money the participant had won or lost. Participants were asked to decide which deck to select on 100 trials, although they were not told in advance how many trials there would be. In addition, a test of skin conductive response was given as means of measuring "emotional response."
The sample was made up of 13 healthy participants and 5 participants with vmPFC damage.
The decks were not random. Decks A and B would return high rewards initially but would then deliver larger and larger losses as the game went on. These decks should, therefore, be identified as ‘bad’, and participants should learn to avoid them through the experience of the game. Decks C and D, by contrast, would deliver small rewards initially but would also have very small losses as the game continued. These decks should, therefore, be identified as ‘good’, and participants should learn to favour them through the experience of the game.
The results showed that control participants (with no brain damage) quickly learned the best strategy while those participants with bilateral damage in the vmPFC did not fare so well. It also showed that the control participants developed anticipatory skin conductive responses to the disadvantageous decks (A and B); however, the vmPFC had a significantly lower anticipatory SCR and no clear difference in SCR between the two conditions.
Not only is emotion an important part of effective decision-making, but increased emotion seems to be one way we can ‘know’ when we are making the right decision - or at least we think we are!
Research in psychology: De Martino et al (2006)
De Martino et al, (2006) aimed to explore the interaction of emotion in a financial decision-making task.
 A volunteer sample of 20 British undergraduates was asked to complete a simple financial decision-making task while brain activity was measured using an fMRI scanner. Information was presented to participants in terms of either a loss (negative frame - you had £50, but have lost £30) or a gain (positive frame –you had £50, and you can keep £20). The outcome in both frames is, in fact, the same - you have £20 you didn’t have before.
A volunteer sample of 20 British undergraduates was asked to complete a simple financial decision-making task while brain activity was measured using an fMRI scanner. Information was presented to participants in terms of either a loss (negative frame - you had £50, but have lost £30) or a gain (positive frame –you had £50, and you can keep £20). The outcome in both frames is, in fact, the same - you have £20 you didn’t have before.
In the positive frame, participants were then offered a chance to gamble (risky option – outcome is unknown) or keep £20 (sure option – a certain ‘win’). In this positive frame, loss aversion predicts that people will prefer the sure option and keep £20 – the risky ‘gamble’ option represents a possible loss.
In the negative frame, participants were offered a chance to gamble (risky option – outcome is unknown) or lose £30 (sure option – a certain ‘loss’). In this negative frame, loss aversion predicts that people will prefer the risky ‘gamble’ option as the ‘sure’ option states a certain loss.
As expected, participants were far more likely to choose to gamble in the negative frame condition, even though the options are in fact exactly the same as in the positive frame.
fMRI results demonstrated an interesting pattern of activity in the amygdala, a part of the brain's limbic system which is regarded as being central to emotion. Participants recorded a significant increase in activity whenever they selected the ‘loss averse’ option, regardless of the frame in use.
A key question for this study is the direction of causality. It is difficult to be sure if the emotion associated with increased activity in the amygdala is guiding decision-making or if it is a consequence of decision making. Either way, it is clear that emotion and decision-making are interacting.
Evaluation of the somatic marker hypothesis
Most of the research done to support this theory uses the Iowa Gambling Task. This raises the question of how robust the theory is in explaining decision-making behaviour.
In one version of this study, (Bechara et al, 1997) the team demonstrated that vmPFC patients continued to select cards from decks A and B even though they had told researchers that they knew these decks were disadvantageous. This may indicate that it is not solely a lack of emotional feedback that leads to the patients' poor decision-making.
Wright and Racow (2017) conducted a computerized test using the wonderfully named Balloon Analogue Risk Task (BART). In this task, the participant was presented with a balloon and offered the chance to earn money by pumping the balloon up by clicking a button. Each click caused the balloon to inflate and money to be added to "the pot", up until some point at which the balloon was overinflated and exploded. Thus, each pump brought greater risk, but also greater potential reward. Although they did find that ‘bad’ decisions, (where participants burst the balloon) did result in increased emotional response - indicated by Galvanic Skin Response - they did not find any evidence that this somatic marker helped participants avoid bad decisions in future tasks.
The Somatic Marker Hypothesis may demonstrate that decision making is improved by access to emotion which is relevant to the specific decision being made, but what about decisions made during periods of intense emotion not connected to the decision itself? Such an approach may be a more useful focus for research into emotion and decision-making in the real world.
ATL: Reflection
McCormick and Telzer (2017) have provided some fMRI evidence that risky decision-making in teenagers could be related to a developmental process where the Medial Prefrontal Cortex (mPFC) is less sensitive to negative feedback – so there is a reduced emotional response to negative outcomes.
Watch the following video where Sarah-Jayne Blackmore talks about the role of the mPFC in teenage behaviour.
Think about the risky behaviours that you engage in. Do you think that what you do is significantly different from what you see adults doing?
What are three things that Blakemore says that you think are important to understanding the role of the frontal cortex in risk-taking behaviour?
Do you think that Blakemore's arguments explain why teenagers engage in ‘riskier’ behaviour? If not, how else could we explain this behaviour?
Checking for understanding
What is the function of the ventromedial prefrontal cortex or vmPFC?
All of the responses above except for the psych IA example have an emotional, physiological component which helps the decision making process. The psych IA decision is made by receiving more information - in this case, from a friend. Even though confusion may have led to certain emotions (including a high level of stress that you were not going to do well on your IA), it was not the emotions that prompted the decision that was made.
Bechara's study of patients with bilateral damage to the vmPFC is an example of
The IV in the study is whether or not the participants have bilateral damage to the vmPFC. This is, therefore, a purposive sample. When the sample is purposive and the differences measured are between those with a trait and without, this is an example of a quasi-experiment.
According to research by de Martino et al (2006), which part of the brain appears to play a role when we have to make a decision which may result in a loss?
Which of the following is a limitation of the study by de Martino on emotion and loss aversion?
Research using the Balloon Analogue Risk Task (BART) shows that
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn