 IB Docs (2) Team
IB Docs (2) Team

Thobois et al (2004)
 In the biological approach, it is argued that behaviours and cognitive processes may be localized in specific parts of the brain. Damage to a part of the brain often gives researchers an insight into the role that it plays in behaviour - including our mental health.
In the biological approach, it is argued that behaviours and cognitive processes may be localized in specific parts of the brain. Damage to a part of the brain often gives researchers an insight into the role that it plays in behaviour - including our mental health.
Thobois et al (2004) carried out a case study on a patient with damage to the caudate nucleus in order to determine its role in the compulsive symptoms of OCD.
The original study may be found here
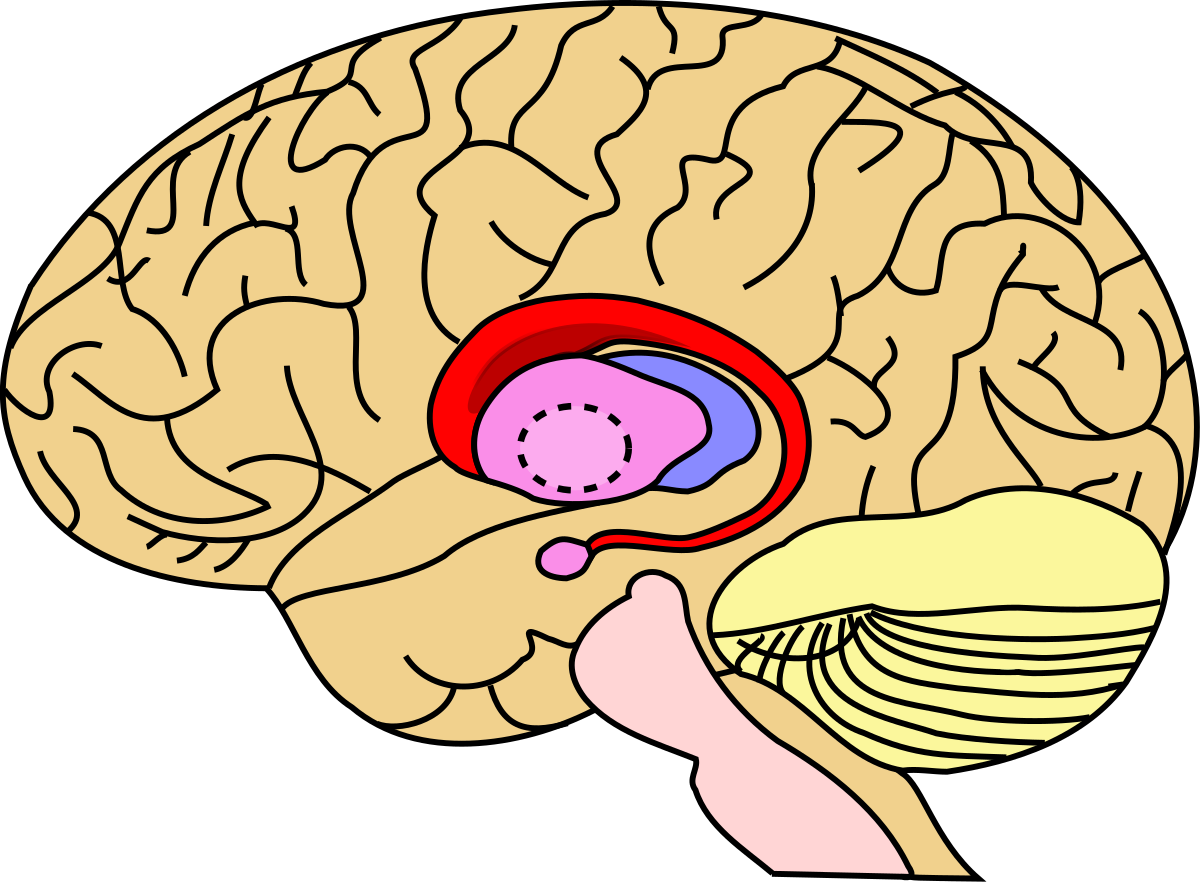
One of the key biological explanations of OCD is known as the worry circuit (Insel, 1992). The worry circuit primarily consists of three parts of the brain: the orbital-frontal cortex, the caudate nucleus, and the thalamus.
The orbital-frontal cortex [OFC] is the part of the brain that notices when something is wrong. For example, when the OFC registers that there is a threat of danger nearby (e.g. something dirty that could lead to infection), it sends a 'worry' signal to the thalamus.
The thalamus interprets these signals and then sends messages to different parts of the brain in order to cope with the threat - in this case, messages are sent back to the OFC. These nerve cell connections form a "circuit" in the brain. The caudate nucleus regulates signals sent between the OFC and the thalamus.
Normally, the caudate nucleus acts like the brake pedal on a car, suppressing the original 'worry' signals sent by the OFC to the thalamus. This prevents the thalamus from becoming hyperactive.
In people living with OCD, the caudate nucleus is thought to be damaged, so it cannot suppress signals from the OFC, allowing the thalamus to become over-excited. If this occurs, the thalamus sends strong signals back to the OFC, which responds by increasing compulsive behaviour and anxiety. This could explain the repetitive and seemingly senseless rituals performed by obsessive-compulsives.
The researchers carried out a case study of a 24-year-old right-handed male who underwent surgery to remove a hematoma (a blood clot caused by broken blood vessels) after a stroke in the region of the caudate nucleus.
Three months later the patient developed compulsive behaviour. He couldn't stop himself from only using words and sentences of 10 letters. He showed no anxiety or obsessive thoughts. He also exhibited signs of aggressiveness. Although he was aware of his OCD symptoms he did not recognize the change in his personality. His symptoms stopped him from going to work and severely impacted his social functioning. Two years later he was referred for further testing. It was at this point, that Thobois et al began their case study.
Procedure
A battery of psychometric tests was used to assess his cognitive abilities including verbal fluency and memory. They also measured his IQ using the Wechsler Adult Intelligence Scale-III (WAIS-III). With regard to psychiatric symptoms, he completed the Beck Depression Scale and the Yale-Brown Obsessive-Compulsive (YBOC) scale.
Findings
The man had normal scores for verbal fluency, e.g. he named 18 words in one minute starting with ‘r’ but poor verbal comprehension (6/19) on the WAIS-III. While his depression score was within the normal range (3/30), his YBOC compulsion score was 12/20 and his obsession score was 0/20. This is consistent with a diagnosis of compulsive behaviour (pure OCD). In addition, the YBOC indicated that the patient spent between 30 minutes and 2 hours a day on his compulsive behaviours and felt the behaviours were beyond his control.
Conclusions
In this case study, the compulsive behaviours could be said to have been triggered by caudate nucleus damage from the stroke and subsequent surgery, as the patient did not suffer any symptoms prior to this.
Strengths
- The case of bleeding in the caudate nucleus is a rare case and provided researchers with a unique opportunity to explore the role of the caudate nucleus in compulsive behaviours.
- The case also differentiated between obsessive and compulsive behaviour as the patient has "pure OCD."
- The researchers used the YBOC scale to measure compulsive behaviours and obsessive thoughts; this scale has been shown to have strong concurrent validity and high inter-rater reliability.
- Cross-case analysis suggests that the findings from this study are reliable.
- It must be remembered that this is a case study of secondary OCD, i.e. where OCD has been acquired after physical trauma to the brain and therefore the findings may not apply when thinking about primary OCD.
- Case study evidence may lack generalisability as the study focuses on just a single individual; his unique life experiences may have influenced his symptoms, i.e. the absence of obsessive thoughts. This is supported by the fact that in Katz and Flemming’s (2014) case study the patient did develop obsessive thoughts around contamination as well as compulsive behaviour.
- As the lesions on the caudate nucleus were naturally occurring as a consequence of a stroke, it is unclear whether any other brain regions were also damaged.
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn