 IB Docs (2) Team
IB Docs (2) Team

Cognitive approach to anorexia
 According to the DSM-V, Anorexia nervosa is characterized by distorted body image and excessive dieting that leads to severe weight loss with a pathological fear of being overweight.
According to the DSM-V, Anorexia nervosa is characterized by distorted body image and excessive dieting that leads to severe weight loss with a pathological fear of being overweight.
Many psychologists argue that eating disorders are not the result of biological factors, but instead are the result of perception - in particular, a false perception of how one's body actually looks.
There are two predominant theories that cognitive theorists study. First, there is a theory that faulty thinking based on schema is the reason for the disorder. Secondly, the theory of attentional bias. However, as you will see, there are many questions that the cognitive approach leaves unanswered.
The role of schema
The cognitive level of analysis focuses on how we process information. One way in which we do this is through our schema. Remember, a schema is a mental representation based on past experience that helps us to understand the world around us. People with eating disorders tend to demonstrate patterns of faulty thinking. For example:
- They perceive themselves as overweight, even when they are underweight.
- They have feelings of low self-worth because of their physical appearance.
- They use dichotomous thinking: I ate one chocolate - I have ruined my figure!
- They overgeneralize: If I cannot control my eating, no one will love me.
- They set unrealistic goals: If I reach a size 2 then life will be perfect.
People living with anorexia appear to have schema that distort their perception of their body image. This leads to the Body-image distortion hypothesis.
Bruch (1962) claimed that many patients with eating disorders suffer from the cognitive delusion that they are overweight. Bruch wrote that anorexics show "an absence of concern about emaciation, even when advanced, and the vigor and stubbornness with which the often gruesome appearance is defended as normal and not too thin (p 189)."
In a study of body-image distortion, Fallon & Rozin (1985) showed nine pictures of different body shapes, from very thin to very heavy, to 475 US undergraduates of both sexes and asked them to do three tasks:
- Show which body shape is most similar to their own shape;
- Show which body shape is most like their ideal body shape;
- Show which body shape of the opposite sex would they be most attracted to.
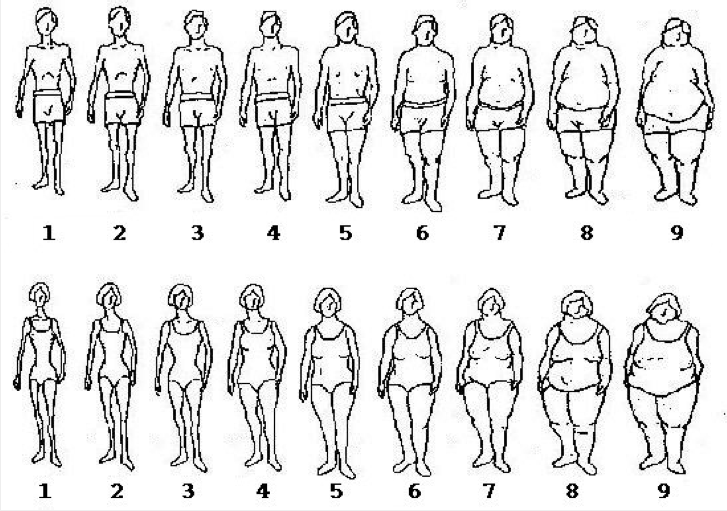
The researchers found a significant difference between men and women. Women often chose shapes that were larger/heavier than their actual body weight. Their ideal body shape was also much thinner than the one they had chosen as similar to their own body shape. Men chose very similar figures for all three body shapes. This could explain why American women have a higher risk for anorexia and bulimia.
Similar to the Fallon & Rozin study, McKenzie et al (1993) interviewed women with eating disorders and a control group about their body weight, shape, and ideals, and got them to estimate their own size in relation to other women. They found that when asked to compare themselves with controls who were the same size, women who had been diagnosed with an eating disorder tended to overestimate their own body weight. When asked to indicate their ideal body weight, women with eating disorders chose a significantly lighter weight than the control group. The participants were then given a chocolate bar and a soft drink to consume. Following this, they were asked to re-estimate their body weight. The women with eating disorders judged that their size has increased, while the control group judged that their size had not changed.
Fairburn (1997) suggested that people with eating disorders had distorted weight-related schema and low self-esteem. These schemas may develop as a result of cultural norming or personal feedback - for example, compliments received as a result of weight loss or being told that she needs to lose weight if she wants to "get the boys." Then the goal becomes to lose weight and to stay thin in order to increase a sense of self-worth. However, the obsession with weight control may lead to depression and feelings of low self-esteem, leading to greater and greater weight loss.
Attentional bias
 Attentional bias is when we focus on certain stimuli and ignore others. When making a decision, we often focus on just a few of the options while we ignore the rest. Psychologists have investigated the role of attentional bias in people living with anorexia nervosa. It is argued that the typical characteristics of perfectionism, attention to detail, and obsession with order may be a result of this cognitive bias. By focusing only on their need to lose weight, they are not looking at the more global effect of their restrictive eating behaviours and the potential outcomes.
Attentional bias is when we focus on certain stimuli and ignore others. When making a decision, we often focus on just a few of the options while we ignore the rest. Psychologists have investigated the role of attentional bias in people living with anorexia nervosa. It is argued that the typical characteristics of perfectionism, attention to detail, and obsession with order may be a result of this cognitive bias. By focusing only on their need to lose weight, they are not looking at the more global effect of their restrictive eating behaviours and the potential outcomes.
Many of the studies of attentional bias have used modified Stroop tests - the "Food Stroop Task" and "Body Stroop Task." Words are displayed one by one on a computer screen and subjects are instructed to name the colour in which every word is printed. The attentional bias is supposed to be reflected in the extent to which the word meanings interfere with the speed of colour naming: The longer it takes to name the colour, the larger the attentional bias.
Stormark & Torkildsen (2004) used a sample that consisted of 20 females with eating disorders (anorexia nervosa, bulimia nervosa, or a combination of both) and 24 female controls. The participants were timed on different versions of the Stroop test: colour, food and neutral stimuli. In addition to giving a Stroop test that used words about food, on another version pictures were used. The eating disorder group was slower than the controls in identifying the colour of all words (including the food words) as well as the pictures depicting food stimuli. The eating disorder group was also slower in identifying the colour of food words and pictures than food-neutral stimuli. This means that women suffering from eating disorders paid more attention to stimuli that involved food than control groups. This over-attention to food-related stimuli may influence their disorder.
Southgate, Tchanturia & Treasure (2008) compared women with anorexia and female controls using a different test - the Matching Familiar Figures Test (MFFT). In this test, an image is shown and then 8 similar images are shown. Subjects have to identify the image that matches the initial image. The researchers found that women with anorexia had a significantly higher rate of accuracy than the other two groups. This demonstrates high attention to detail.
Theoretically, if people who suffer from anorexia pay more attention to stimuli that are related to food and body image, then therapy could try to change these attention patterns. A recent study by Kim et al (2014) went a step further. The study found that oxytocin decreases anorexic patients’ tendencies to fixate on images of high-calorie foods and larger body shape.
In their study, 31 patients with anorexia and 33 healthy controls were given either a dose of oxytocin, delivered via nasal spray or a placebo. The participants were then asked to look at sequences of images relating to food (high and low calorie), body shape (fat and thin), and weight (scales). Once the images flashed on the screen, the researchers measured how quickly participants identified the images. If they had a tendency to focus on the negative images, they would identify them more rapidly. The test was done before and after taking oxytocin or placebo.
After taking oxytocin, patients with anorexia reduced their attentional bias on images of food and fat body parts. This theory will require more research, but it does appear that there may be a biological link to the attentional biases seen in people living with anorexia.
ATL: Critical thinking
There are several studies in this section on the cognitive origins of anorexia nervosa. Which study do you feel is the "strongest" in supporting the claim that cognitive factors lead to anorexia? Which study do you think is the weakest? Be able to support your position.
In order to answer this question, students should consider the different ways that we evaluate research. In this case, the question is asking which one makes the strongest connection between cognitive factors and anorexia, so ethical considerations will be rather irrelevant. Below are some evaluation points for the studies on this page, but the question as to which is the strongest/weakest is up to students to defend.
You may want to have students work in groups. The group may look at all five studies, but this is a bit much. So, you may want to have each group focus on one study. Then have groups paired - so, pair McKenzie with Kim and have them decide which group has the strongest study. Have them continue to do this until they have spoken with each of the groups and then have the class make a final decision. If you are going to use this second approach, you may want to leave out one of the studies below to have an even number to work with.
At the end of the conversation, students should be able to talk about the general limitations of cognitive research on eating disorders.
Fallon & Rozin (1985) The sample is highly problematic in this study. The undergraduates are not representative of the general population and they do not represent a population of people with eating disorders. The images that were used were not images of real people, making this a rather artificial experience. It is a rather significant assumption that this is an explanation of why people go on to develop eating disorders.
McKenzie et al (1993) This study seems to support, to some extent, the findings of Fallon & Rozin. The use of a sample with diagnosed eating disorders and a control of healthy participants makes the study more generalizable to these populations. The task is still artificial, but the experiment is well controlled so there is high internal validity. In addition, the second part of the experiment allows the researcher to compare participants' responses to previous responses. This study is a mixed design - both independent samples and repeated measures.
Stormark & Torkildsen (2004) This study is really interesting, but it doesn't tell us whether the attentional bias is the cause of the disorder or a symptom of the disorder. The study is highly controlled, so it has high internal validity, but again, the task is highly artificial. The sample is made up of people with the disorder and is not an analogous sample. This increases the study's population validity.
Southgate, Tchanturia & Treasure (2008) See comments on Stork & Torkildsen (2004).
Kim et al (2014) This is an interesting study because it uses theory triangulation. The study has high internal validity and low ecological validity.
- Patterns of faulty thinking may be a symptom of the disorder, rather than an actual cause of the disorder.
- Many people are dissatisfied with their bodies but do not develop an eating disorder. Cognitive arguments do not explain this individual difference.
- In studies of attentional bias, many investigators have generated their own Stroop word lists of various lengths and with various properties. Few of these word lists have been standardized.
- Samples are defined by a previous diagnosis, rather than the symptoms and their severity. Therefore, it is difficult to draw conclusions.
- Cognitive behavioural therapy has been rather successful in the treatment of anorexia. This implies that faulty thinking and body image schema may play a key role in the disorder.
Checking for understanding
1. What does it mean when we say that people living with anorexia "engage in patterns of faulty thinking?"
Faulty thinking is thoughts that cause individuals to perceive reality inaccurately. These thinking patterns often are said to reinforce negative thoughts or emotions. Faulty thinking tends to interfere with the way a person perceives an event. In the case of people living with anorexia, this thinking is related to food and eating.
2. What is the key problem with the sample used in Fallon & Rozin's study?
The key problem is that the sample did not include women with eating disorders. The study did find gender differences in body image perception and ideal body image - and it was argued that this may account for the gender differences in eating disorders. The correlational data here is being generalized to a theory of eating disorders but lacks direct evidence in the eating disorder population.
3. According to Fairburn, how do weight-related schema develop?
The same way that all schema develop - through one's personal experience of interacting with one's culture and environment.
4. What do the results of Stormark & Torkildsen's seem to indicate?
It seems to indicate that individuals with eating disorders pay more attention to weight and food than the average person.
5. What is a general problem with the samples used in research on people living with eating disorders?
Often, all eating disorders are considered in a single sample. This is, as seen in the video above because often individuals go through periods of anorexia and bulimia. There is no control of the level of the symptoms and often the samples are not matched for variables such as sexual abuse. In addition, most research has been done in the West, so the samples are also culturally biased.
Exam tips
The question on the exam would most likely be "Evaluate one or more cognitive explanations of one disorder." When answering this question, you should:
- Define key terms: faulty thinking, schema, attentional bias.
- Describe 2 - 3 studies which demonstrate the role of cognitive factors. You could either describe a few studies that look at schema theory or one of schema theory and one on attentional bias.
- Evaluate the studies.
- Discuss the strengths and limitations of a cognitive argument about the nature of eating disorders.
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn