 IB Docs (2) Team
IB Docs (2) Team

Lopatka and Rachman (1995)
 The cognitive approach argues that behaviour is determined by the way we process information and thus abnormal behaviour must stem from faulty thinking strategies. Salkovskis argues that compulsive behaviour stems from an inflated sense of responsibility for negative outcomes.
The cognitive approach argues that behaviour is determined by the way we process information and thus abnormal behaviour must stem from faulty thinking strategies. Salkovskis argues that compulsive behaviour stems from an inflated sense of responsibility for negative outcomes.
The abstract of the original study can be found here.
The cognitive approach argues that "patterns of thinking" often lead to behaviour. In the study of abnormal psychology, cognitive theorists often talk about "irrational thoughts" or dysfunctional thinking patterns.
Schema are mental representations based on past experience that helps us to interpret information in our environment. A highly controlling parent, bullying, or a high-stress home environment may all lead to maladaptive schema - that is, a cognitive framework that may distort the thinking of an individual about a situation. Salkovskis argues that this schema is one of "personal responsibility" in which individuals see themselves as responsible for the safety of others - and a sense of shame or ineptness for having thoughts that may compromise others' safety.
The following study tested Salkovskis’ cognitive theory of OCD by manipulating perceived responsibility to see how this affected compulsive checking and cleaning behaviour in people diagnosed with OCD.
Volunteer sampling was used to gather 30 compulsive checkers. They were recruited from clinics, newspapers, radio/television adverts, and notices posted on bulletin boards in hospitals and 'self-help' bookstores.
There were two experimental conditions:
Low responsibility condition: Participants were told that the researcher would take full responsibility for anything that was not perfect, or if something bad were to happen, that the researcher would pay for any damage. All of this was then put into a contract signed by both the researcher and the participant to ensure that the participant was absolutely clear that they were in no way responsible.
High responsibility condition: Very similar wording was used as in the low responsibility condition to standardize the instructions provided across the two conditions, but they were told that they must take full responsibility for anything that was not perfect and that for any bad outcomes the participant must pay for any damage. Again, everything was put in writing, with both parties having to sign the contract.
There was also a control condition. The participants were asked to treat the situation as they would in everyday life and that the researchers were simply interested in learning more about their regular checking in everyday situations.
The study used a repeated measures design using counterbalancing. Participants took part in all three levels of the independent variable: high and low perceived responsibility, and a control condition. The dependent variables were self-reported discomfort, urge to check, and perceived responsibility to check the manipulation of the independent variable had worked.
The checking/cleaning situations varied according to each individual participant’s compulsions, e.g. they were told “Without checking it at all, we would like you to:
lock the door and then walk away from it;
turn the stove on and then off and then walk into the next room;
adjust the thermostat to 20°and then walk into the next room.
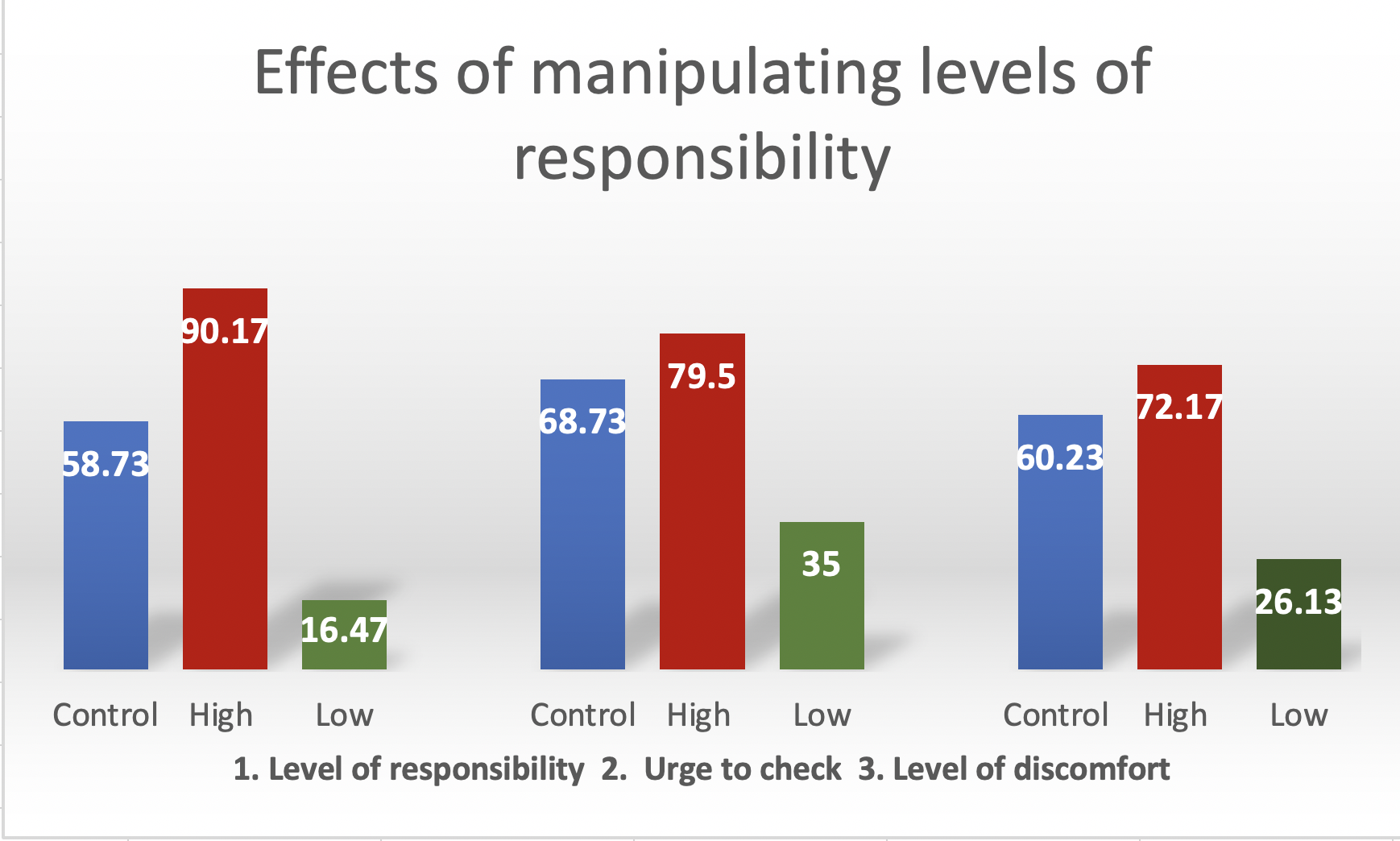
As can be seen in the graph above, the average urge to check went down from 68.7 in the control condition to 35 in the low responsibility condition, with similar decreases in discomfort. In each instance, the self-reported percentage roughly halved. Increasing responsibility also led to change in the expected direction but the differences were not as great, e.g. the urge to check went up by 10 points from 69 to 79.5, and discomfort by 12 points from 60 to 72. The researchers note that this may have been due to the fact that the participants already experienced high levels of distress and urges to check.
The researcher notes this interesting cognitive distortion for people with OCD, i.e. that they overestimate the risk of a negative outcome when they feel responsible, but that bad outcomes are less likely when someone else is responsible.
The use of the repeated measures with counterbalancing is a strength as this design helped minimize participant variables and order effects. However, participants always experienced the control conditions first; this may reduce internal validity.
The assistant who conducted the self-report measures was blind to the condition and main hypotheses of the study, reducing the likelihood of researcher bias.
The experiment was conducted in the participants' own homes adding ecological validity to the testing environment. This is a strength as people with OCD may behave differently in their homes than they would in an unfamiliar environment.
The study used the DSM-IIIR criteria in order to ensure participants had symptoms that were severe enough for inclusion in the study; this means the results may no longer be valid as the classification of OCD in the DSM 5 has changed significantly since this version.
The study only tells us about checking compulsions and many people with OCD have other types of compulsions, for example, ordering and/or counting.
The study only included self-reported data and is thus reliant on the person’s ability to report their symptoms accurately and honestly; participants may have been responding to demand characteristics - that is, they knew they were meant to report reductions in symptoms when responsibility was lower.
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn