 IB Docs (2) Team
IB Docs (2) Team

Health promotion

Essential understandings
Health psychologists employ different models to affect change in people's health related behaviours.
There are difficulties in assessing the effectiveness of health promotion campaigns.
An important part of health psychology is to put theory into practice in health promotion. Psychologists assume that one way to change unhealthy behaviours is to change attitudes and beliefs. The main goal in prevention programs is to encourage people to change their health-threatening behaviours, or to prevent people from developing health-threatening behaviours in the first place. This is not as easy as it sounds because the exact link between beliefs and behaviours is not known. Another problem is that at the time that health-threatening behaviours develop, people often have very little immediate incentive to change their behaviours. For example, problems related to smoking occur many years after people have taken up smoking, not when they start the habit.
There are several strategies to try to change the health behaviours of either an individual or a whole population. As you can probably guess, these models do not work for everyone, but in order to be effective, they should be able to produce a noticeable and enduring change in a significant percentage of the population.
Health psychologists often base interventions on theories and empirical research related to decision making, in order to understand what factors contribute to people’s decisions to change. Two important theories on decision making that have guided interventions are the Health Belief Model (HBM) and Social Cognitive Theory.
ATL: Thinking critically
In the world of non-stop information, it is difficult to believe that the average person does not know that some behaviours are bad for their health. In most countries, for example, cigarettes are clearly labeled with a warning that says that Cigarette Smoking Causes Cancer. In spite of this, people continue to smoke. Why?
Such examples show that we human beings are very good at discounting the threats that their behaviours cause to their health.
Watch the following video. What do you think? Will this change a smoker's behaviour? Why or why not?
There are two aspects of this promotion and students tend to focus only on one - the people in the video who get the note from the children. Could this have an effect on these people? Potentially. However, as the people in this video clearly know that smoking is bad for them, it is not clear that they will necessarily change their behaviour. What increases the potential for change is that in that moment of doubt about their behaviour brought on by the child's note, there is a phone number where they can get help. The sooner they call the number, the greater the chance of change. Planning to "call later" will allow for rationalization and most likely not result in any change in behaviour.
But this campaign was designed to change the viewers' behaviours. This aspect of the campaign is often lost on the students. To be frank, we cannot know from watching the video that the people in the video are not actors! (By the way, they weren't.) Watching this video at home may mean that people are more likely to call the number - they are in the privacy of their home and their phone is easily available.
The Health Belief Model
The HBM and is one of the oldest social cognition models. The HBM predicts that individuals will take a health-related action if they think that a negative health problem - for example, developing lung cancer or type 2 diabetes - can be avoided by taking the recommended action and that they will be successful in doing so.
It is based on the assumption that for a behavioural change to succeed, individuals must have the incentive to change, feel threatened by their current behaviour, and feel that a change will be beneficial and be at an acceptable cost. They must also feel competent to implement that change.
The HBM sees people as rational and suggests that the likelihood that a person will engage in healthy behaviour depends on a number of factors, such as:
Evaluation of threat - for example, being overweight may result in developing a heart condition; smoking may result in lung cancer. The person will probably recognize this as a serious condition, but may also believe that it does not happen to people like them, for example, people their age. The model claims that people only act if they perceive a threat - for example, a physical symptom like chest pains, death of somebody from heart disease or lung cancer, or information from a mass media campaign.
Cost-benefit analysis - the person will evaluate whether the perceived benefits will be higher than the perceived barriers - for example, if you have to buy healthy food, this is more expensive than chips and burgers.
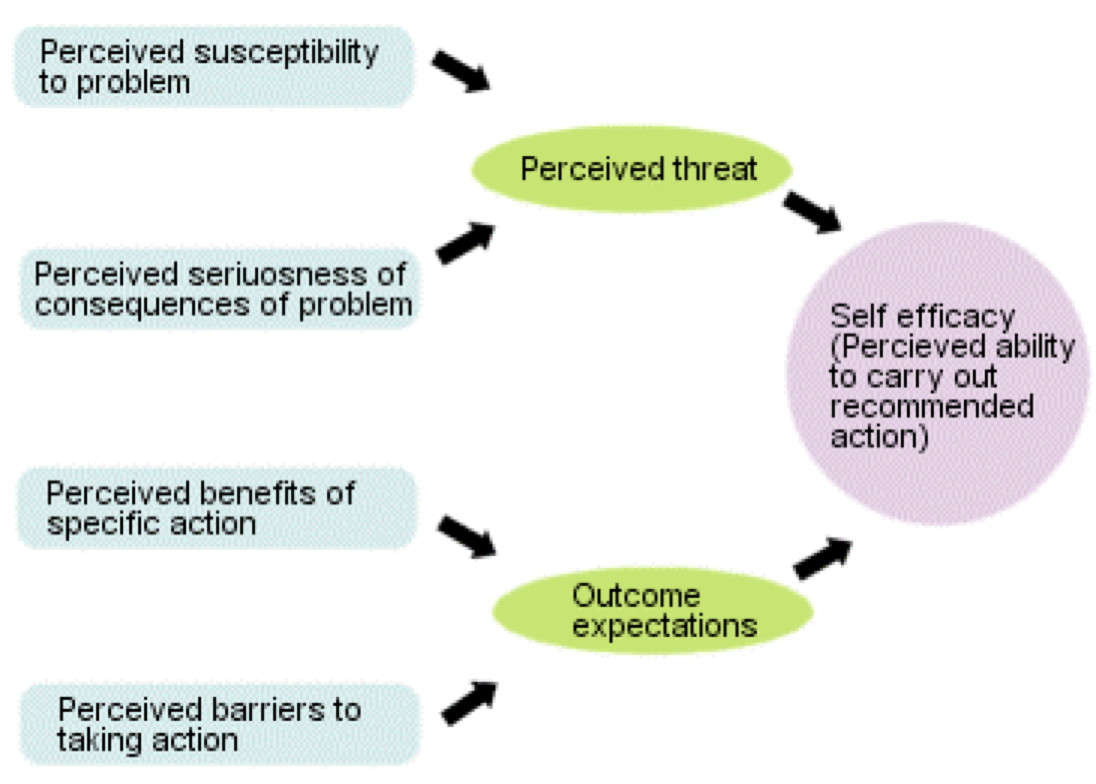 The HBM model also includes self-efficacy beliefs - that is, the belief that you can perform adequately in a particular situation. This feeling of competence will influence perception, motivation, and performance. Bandura (1977) suggested that self-efficacy beliefs are important predictors of what people believe they are capable of. People make judgments of self-efficacy primarily on the basis of previous achievements. Other sources of judgment include:
The HBM model also includes self-efficacy beliefs - that is, the belief that you can perform adequately in a particular situation. This feeling of competence will influence perception, motivation, and performance. Bandura (1977) suggested that self-efficacy beliefs are important predictors of what people believe they are capable of. People make judgments of self-efficacy primarily on the basis of previous achievements. Other sources of judgment include:
- Observations of the performance of others - If he can do it, so can I!
- Social and self-persuasion - You can do it!
- Monitoring emotional states - for example, feeling anxious suggests low expectations of efficacy.
The Health Belief Model argues that a person's "readiness to change" is based on five factors. An example of how these factors can be applied can be seen in campaigns to promote the use of condoms to avoid HIV infection.
Perceived vulnerability: People have to believe that they can get HIV and know how one contracts the disease.
Perceived severity: People need to believe that the consequences of getting HIV are significant enough that they want to avoid contracting it. This is often accomplished through fear arousal.
Perceived benefits: People have to understand the benefit of using condoms to avoid HIV infection.
Perceived barriers: Barriers need to be explicitly identified and plans need to be developed to overcome them. People may be embarrassed to ask a partner to use a condom or they might not want to pay to buy condoms. So, for example, practicing condom communication skills or informing them about where they can get free condoms would potentially be successful strategies.
Cues to action: People need to be reminded of safe sex practice in newsletters, a conversation with a friend or receiving a pin that says "no glove, no love" or "respect wears a condom."
Research in psychology: Quist-Paulsen et al. (2003)
 Quist-Paulsen et al. (2003) conducted a field experiment in which they investigated patients who had been treated for heart problems in a Norwegian hospital. It is known that mortality is reduced by 50 percent beyond three to five years if such patients stop smoking. Normally, 30 - 45 percent of heart patients will stop spontaneously after treatment for cardiovascular problems.
Quist-Paulsen et al. (2003) conducted a field experiment in which they investigated patients who had been treated for heart problems in a Norwegian hospital. It is known that mortality is reduced by 50 percent beyond three to five years if such patients stop smoking. Normally, 30 - 45 percent of heart patients will stop spontaneously after treatment for cardiovascular problems.
The researchers wanted to see if a longer intervention, including fear arousal, would get more people to stop smoking and prevent relapse. They randomly assigned participants to a treatment group and a control group. All patients were offered group counseling sessions. Patients in the control group received no further counseling on how to stop smoking.
Patients in the treatment group had personal advice from trained nurses and received material that stressed the risks of continued smoking and the improved outcomes of cessation. Patients were advised to stop, and nicotine replacement was offered to those with cravings. Spouses were also advised to stop smoking.
The nurses contacted the patients nine times after they went home, to encourage them to stop smoking. They stressed the negative aspects of smoking on their condition. Patients also had two consultations in the year after leaving the hospital. The researchers found that 57 percent of the intervention group and 37 percent of the control group had stopped smoking. They concluded that the program based on fear arousal and relapse prevention was effective for this group of patients.
ATL: Inquiry
 When discussing health choices, it is not just about smoking. It is about sex safe, drug and alcohol use, diet choices, exercise routines, and stress management. For this task, you are going to be asked to find out if there is a disconnect between health beliefs (or knowledge) and actual behaviour.
When discussing health choices, it is not just about smoking. It is about sex safe, drug and alcohol use, diet choices, exercise routines, and stress management. For this task, you are going to be asked to find out if there is a disconnect between health beliefs (or knowledge) and actual behaviour.
To do this, we are going to create a short survey and then quantify and represent our data.
Step 1. Develop a survey with the goal of finding out how much people exercise compared to what they know about the health benefits of exercise.
Step 2. Carry out the surveys. If a participant reads your whole survey before answering, there may be strong expectancy effects. Therefore, it would be best for you to carry out the survey orally. Try to find five people to interview. If possible, avoid interviewing fellow students.
Step 3. Now it's time to graph your data as a class. There are many ways that you can do this based on how you wrote your survey. For example, in the survey I designed, I asked how many times they exercised per week on a regular basis and then asked them to name as many health benefits of exercise that they knew. So, for my graph, I am going to make my x-axis the number of times that they exercise per week and the y-axis the number of correct health benefits that were identified.
To make my graph, I can use a simple online tool like "scatter plot generator." When I enter my data and choose linear regression, it may look like this:
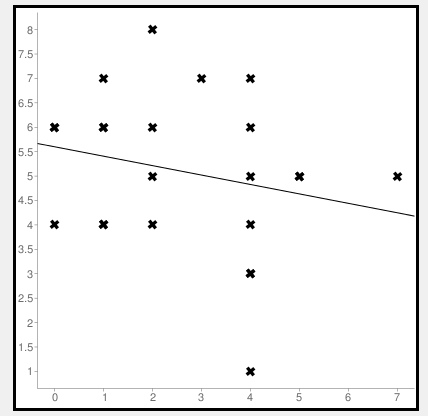
As you can see from the graph and the line of best fit, there is a very minimal link between the two variables. In order to actually see the level of correlational, click on the "correlation coefficient." This is a calculation of the Pearson's r test. When I do my calculation, I find that the correlational coefficient for my data is r = -0.23. This means two things. A value of 1.0 would mean a very strong correlation - that is, that those that know more about exercise do more exercise. In this case, it is only .23. So there is only a very weak correlation. Secondly, you can see the negative sign. This indicates the direction of the correlation. In this case, it appears that there is a very slight correlation in the direction that those that exercise more know less about the health benefits.
How does your data compare to mine?
A problem in the HBM is the focus on individual cognitions. It does not include emotional, social, and economic factors, which are known to influence health behaviours as well. It seems difficult to make standard measurements of many of the concepts - for example, perceived vulnerability.
The HBM is also criticized for assuming that people are rational, which is not always the case. Research has found that awareness of health risks alone does not necessarily inhibit people from engaging in potentially risky behaviour. Studies have found that people are quite optimistic about their health. Weinstein (1987) asked people to rate their risk of developing various disorders compared to people like them. Individuals usually rate their chances of illness as lower than for other people. This is the case in smokers, to a large extent. Weinstein suggested that the following factors affect “unrealistic optimism”.
- People tend to believe that if a problem has not appeared yet, then it is unlikely to happen in the future.
- People tend to think that personal action can prevent the problem.
- People believe that the problem is rare.
- People have little or no experience of the problem.
The Health Belief Model has been successfully applied in many cases to change behaviours from as varied as smoking to safe sex to dietary change to prevent type II diabetes.
However, the HBM ignores the role of social and environmental factors on health, such as peer pressure and cultural norms.
Finally, the model assumes that health behaviour change can happen simply by conscious choice. This may not always be the case. People suffering from nicotine addiction often want to quit, but simply cannot. Since health behaviour is seen solely as a choice, there is the temptation to "blame the victim" rather than recognizing the complexities of changing behaviour.
Social Cognitive Theory
Social Cognitive Theory suggests that health promoters act as ‘change agents’, facilitating change through modification of the social environment and the development of skills and capacities that enable individuals to make healthy changes. If you remember from the core, there are several important components of Social Cognitive Theory.
Observational learning is the ability to learn by observing the behaviour of others. For example, people may be more likely to follow the example of people they see as role models. Seeing someone you respect refuse to eat unhealthy foods may, therefore, change your attitude about what you eat.
Expectations are the value an individual places on the outcomes resulting from different behaviours. For example, if you believe that smoking will help you to lose weight and place great value on weight loss, then you may be more likely to take up smoking.
Reciprocal determinism describes the way in which behaviour and the environment continuously interact and influence one another. This is a key difference between this theory and the Health Belief Model. Social Cognitive Theory stresses the need for addressing environmental influences in order to promote change. For example, modifying social norms about smoking is considered to be one of the most powerful ways of promoting cessation among adults.
Self-efficacy is an individual’s belief and level of confidence in her/his own ability to successfully make a change or perform a behaviour. Social cognitive theory identifies self-efficacy as the most important factor for successful change.
Health promotion campaigns that are based on Social Cognitive Theory include an informational component to increase perceptions of the risks and benefits associated with a particular behavior, teaching social and cognitive skills that can be used to initiate behavior change, building self-efficacy to promote behavior maintenance, and building social support to sustain change.

The first attempt at applying the Sabido Method was in a soap opera called Acompáñame ("Accompany Me"). The results of Acompáñame, as reported by the Mexican government's national population council (CONAPO), were:
- Phone calls to the CONAPO requesting family planning information increased from zero to an average of 500 a month. Many people calling mentioned that they were encouraged to do so by the television soap opera.
- More than 2,000 women registered as voluntary workers in the national program of family planning. This was an idea suggested in the television soap opera.
- Contraceptive sales increased 23 percent in one year, compared to a seven percent increase in the preceding year.
- More than 560,000 women enrolled in family planning clinics, an increase of 33 percent (compared to a one percent decrease the previous year).
The Sabido method is based on several of the factors that promote social learning:
- Because viewers are committed to watching the show, they pay attention and retain the plot.
- They observe both the rewards and punishments that are received by the characters for the choices that they make – that is, vicarious reinforcement.
- They identify with the characters and feel connected to them. This serves as motivation to replicate the behavior.
- The characters in the soap opera are “average people”- many viewers will see them as part of their in-group.
The Sabido method has been successfully applied in other countries. For example, from 1993 to 1997 there was a serial in Tanzania to promote AIDS prevention behavior, the ideal age of marriage for women, and the use of family planning. In order to test the effectiveness of the program, a nationwide program was set up with the assistance of the University of New Mexico. The experiment used an independent samples design. In the area near the capital city of Dodoma, a music program was played. This was the control. The rest of the country heard the serial broadcast by Radio Tanzania. The program ran for two years.
Nationwide surveys showed a significant increase in the percentage of listeners in the broadcast areas who believed that they were vulnerable to HIV infection; an increase in the belief that audience members, rather than their God or fate, can determine how many children they will have; and an increase in the percentage of respondents who approve of family planning. Importantly, the research showed a very significant increase in family planning use and a reduction in fertility rate only where the program was broadcast (Vaughan et al, 2000).
ATL: Critical thinking
Watch the following video. In what ways does this campaign use Social Cognitive Theory to change behaviour? Do you think that this campaign would be successful in increasing the use of sun protection? Why or why not?
This campaign plays to one's emotions - especially about the love between a parent and child. This is the focus of the potential change for the parents in the video who realize that they are not acting in the best interest of their children by not requiring them to wear a hat or sun cream.
However, it is the viewer of the campaign that is influenced by SCT. Watching the video, they observe the negative experience of the parents, realizing that they are potentially endangering their children. This leads to a sense of "vicarious punishment", where the viewer feels that same sense of shame if they are engaging in the same behaviour. In addition, the campaign is memorable (retention) and catches one's attention. Finally, the people in the campaign are relatable - that is, the people in the audience can identify with them. The people in the video also represent the diversity of the population.
Unlike the Health Belief Model, the Social Cognitive Theory includes environmental factors and seeks to change social norms. Programs such as the Sabido Method have been effective in changing behaviour.
The theory does have limitations. It does not explain why some people choose to change while others do not. It is difficult to measure levels of "self-efficacy." In many studies on the effectiveness of social cognitive theory, self-efficacy has not shown to be a valid predictor of behavioural change.
Checking for understanding
1. According to the Health Belief Model, what would be a perceived barrier to a healthy exercise regime?
A perceived barrier could be that there is not enough time to get to the gym, that gym memberships are expensive or that there are health problems that may prevent all types of exercise. The Health Belief Model gets people to identify the barriers that are preventing healthy behaviour and find a way to address them.
2. To what extent can the Health Belief Model predict behavioural change?
Research seems to support the idea that perceived benefits and barriers can be used successfully to promote healthy behaviour. Simply knowing about the risk or about the severity of a problem does not appear to be as successful in predicting change. Often individuals display an "optimism bias" that their behaviour is healthier than it actually is, and that the risk to them is lower than the general population.
3. What is one ethical concern about the Health Belief Model?
One ethical concern is that the model makes it appear that all negative health behaviours can be changed simply by choice. This is not true and thus may result in feelings of helplessness by individuals or blaming them for their failure. Another concern is the use of fear arousal in order to increase the perception of severity. This may cause undue stress and harm, especially if the individual lacks the resources to change his/her own behaviour.
4. What is Bandura's concept of Reciprocal Determinism?
This is the idea that behaviour affects the environment and the environment affects behaviour in a bidirectional relationship. This is an important part of Social Cognitive Theory as it acknowledges the role that environmental and social factors may play in changing one's behaviour.
5. What are the key differences between the Health Belief Model and the Social Cognitive Theory approach to health promotion?
Social Cognitive Theory addresses environmental factors. It also takes out the role of conscious decision making in changing behaviour. Social Cognitive Theory also emphasizes the need for role models - or "change agents." The theory also encourages the teaching of social and cognitive skills that can be used to initiate behaviour change, build self-efficacy to promote behaviour maintenance and build social support to sustain change.
6. What is one example of a successful SCT-based campaign?
The Sabido method was successfully applied from 1993 to 1997 in Tanzania to promote AIDS prevention behaviour. In order to test the effectiveness of the program, a nationwide program was set up. The experiment used an independent samples design. In the area near the capital city of Dodoma, a music program was played. This was the control. The rest of the country heard the serial broadcast by Radio Tanzania.
Two years later, Tanzanians were more likely to believe that unprotected sex could result in HIV infection, talked more about AIDS, reduced their number of sexual partners and increased condom use.
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn