 IB Docs (2) Team
IB Docs (2) Team

PTSD: Psychological treatments
 Psychological approaches to the treatment of PTSD come in many forms. These approaches are called psychotherapies; they involve face-to-face interactions with a therapist. Psychotherapy is seen as more personal than drug therapy and can be highly individualized to meet the needs of the client. Generally, psychotherapy is more focused on addressing a person's life situation and subjective understanding of his or her psychological problems. Psychotherapy helps people identify unhealthy thought patterns and behaviours as well as suggesting strategies to manage stress and symptoms. A therapist often works with an individual alone, but may also include family members in therapy sessions.
Psychological approaches to the treatment of PTSD come in many forms. These approaches are called psychotherapies; they involve face-to-face interactions with a therapist. Psychotherapy is seen as more personal than drug therapy and can be highly individualized to meet the needs of the client. Generally, psychotherapy is more focused on addressing a person's life situation and subjective understanding of his or her psychological problems. Psychotherapy helps people identify unhealthy thought patterns and behaviours as well as suggesting strategies to manage stress and symptoms. A therapist often works with an individual alone, but may also include family members in therapy sessions.
Testimonial therapy
The following video gives you an example of integrative testimonial therapy as practiced in Cambodia with victims of the Khmer Rouge regime. Watch the video before reading the research below.
Testimonial therapy, also known as narrative exposure therapy, has the goal of helping individuals cope with the trauma that has led to their PTSD symptoms. The key assumption of this type of therapy is that if the client can give meaning to the trauma, then the anxiety and depression associated with it will be alleviated. An essential component of integrative testimonial therapy is the creation of an oral history archive to collect, study, and disseminate the survivors’ memories. This gives meaning and purpose to the experience of the survivor. The therapy provides a time for an individual to look back over and reconsider his or her previous attitudes concerning identity, forgiveness, and violence. It also allows survivors to consider how their experience has affected how they feel about their lives today.
The therapy also works through the process of habituation - that is, by telling their story over and over with the goal of creating an autobiography of the trauma, there is a decrease in their response to the trauma after being repeatedly exposed to it.
In his work with Bosnian refugees, Weine (1998) used testimonial therapy as a means of helping patients overcome their PTSD. In Weine's study, all clients were diagnosed by using the PTSD symptom scale, which had been translated into Bosnian. All testimonies were conducted in Bosnian, translated into English, and then translated back so that the interpreter and the survivor could together correct mistakes and add possible new recollections and details. The final document was given back to the survivor at the final session, and the survivor verified that the document was an accurate reflection of his testimony – increasing its credibility. There are many survivors who do not seek or accept psychiatric treatment from a clinician but who would participate in testimony psychotherapy in the community. Weine found that the rate of PTSD decreased from 100 percent at pre-testimony to 75 percent post-testimony, 70 percent at 2-month follow up, and 53 percent at 6-month follow-up.
Knaevelsrud et al (2014) carried out a study of 30 elderly survivors of World War II (17 females and 13 males) who had been diagnosed with PTSD. The participants took part in an online testimonial therapy program for 6 weeks. Participants were asked to complete two 45-minute writing assignments per week during a 6-week period. Therapists provided the participants with feedback including acknowledgment of the courage to disclose experiences, positive feedback, and frequent encouragement of participants to voice their questions and doubts.
The participants showed a significant decrease in PTSD symptoms and improvement in self-efficacy. In a follow-up interview, all clients had maintained their level of improvement. Only 13% of the participants dropped out of the study.
Firefighters are exposed to many traumatic events. Alghamdi et al (2014) investigated whether testimonial therapy would be effective in the treatment of 34 traumatized Saudi firefighters. Participants were randomly allocated to either a testimonial therapy condition or a "waiting list" control.
The testimonial therapy group received four sessions over a three-week period. The waiting list group received the treatment after a three-week waiting period. Participants in both groups were assessed before the therapy, immediately after the therapy, and at 3 and 6-month follow-ups. The study found a significant reduction in PTSD in the testimonial therapy group compared to the control. After receiving treatment, the waiting list group showed the same improvements as the testimonial therapy group. However, at six months, the majority of the participants had relapsed.
Why is there a difference in long-term effectiveness in the Alghamdi et al (2014) study and Weine's research? A key difference in the two samples was that the refugees were no longer in Bosnia experiencing war, whereas the Saudi firefighters were still on active duty. In the time between the treatment and the follow-up, heavy rains and floods affected many parts of Saudi Arabia and some dams collapsed - requiring firefighters to work up to 24 hours to address the disaster. This stimulus most likely served as a trigger for further PTSD symptoms.
ATL: Critical thinking
Watch the following video on the treatment of PTSD in war veterans.
Much of the research on PTSD is focused on war veterans. After listening to their stories, do you think that their experience is similar to people with other forms of trauma? If so, in what ways?
Do you think that the nature of the trauma would play a role in how the therapy is done?
Much of the research on PTSD is focused on war veterans. After listening to their stories, do you think that their experience is similar to people with other forms of trauma? If so, in what ways?
There are some similarities to people with other forms of trauma. For example, feelings of guilt and failure are common. In addition, a sense of loss is important in trauma. However, unlike other forms of trauma, the military go into their profession knowing that combat is dangerous and that they or their friends may be killed. This is not the same as a victim of rape or someone who had an accident that results in physical harm or disability.
Do you think that the nature of the trauma would play a role in how the therapy is done?
As is seen in this unit, virtual reality therapy has been done to help veterans cope with PTSD. This, however, would not be an appropriate strategy for helping a victim of rape or domestic violence.
Strengths
- There is empirical support for the treatment's effectiveness. For example, Lely et al (2019) carried out a meta-analysis of 16 randomized controlled trials, involving 947 participants. The researchers concluded that NET is effective in the reduction of PTSD and depression symptoms across diverse, predominantly war-affected refugee populations. Treatment results were better for older adults.
- The approach is holistic, rather than reductionist.
- There is cross-cultural evidence to support the effectiveness of the research.
Limitations
- It is difficult to evaluate NET as the therapy is not highly standardized; it is personalized based on the needs of the client.
- The research uses volunteer samples that are already interested in the idea of "telling their story." This may lead to sampling bias.
- The goal of the therapy is to give meaning to trauma. It may be the case that this therapy is not effective in all forms of trauma.
Virtual reality exposure therapy
Virtual Reality Exposure Therapy (VRET) is also based on the concept of habituation. The idea is to disconnect the memory of the trauma from everyday things that can trigger fear and panic. Virtual reality exposure therapy immerses the patient gradually, one stimulus at a time. First, for example, if working with an Iraqi war veteran, the therapist may simply expose the veteran to the sound of the Arabic language. Once that is habituated - that is, when the veteran no longer shows a stress reaction to the sound of Arabic - then other sounds and images can be used.
Watch the following video on virtual reality exposure therapy before reading the research below.
Research in psychology: Difede and Hoffman (2002)
 Difede and Hoffman carried out a case study of a 26-year-old single African American female patient with PTSD. The patient, an executive for a large financial institution, had just stepped out of a drug store across the street from the World Trade Center when the first plane hit on September 11, 2001.
Difede and Hoffman carried out a case study of a 26-year-old single African American female patient with PTSD. The patient, an executive for a large financial institution, had just stepped out of a drug store across the street from the World Trade Center when the first plane hit on September 11, 2001.
The patient went through a series of 9 sessions of VRET, each lasting from 45 to 60 minutes. In each session, the patient would put on head-gear which exposed her to stimuli related to the trauma.
During the therapy, the therapist controlled what the patient saw and talked with the patient about what she was seeing. When the patient was ready, the next stimulus was shown.
The sequence of events to which the patient was exposed included a jet flying over the WTC towers without crashing; the jet hitting the building but no explosion, the jet crashes with an explosion but no other sound effects, the burning building with people screaming and the collapse of the tower. Altogether there were 11 experiences in the sequence.
During the therapy, the patient cried as she told her story of the events of that day - many of which she had forgotten up until VRET. For example, she remembered seeing a woman who was severely injured and begged her for help. She remembered telling the woman that she couldn't stop.
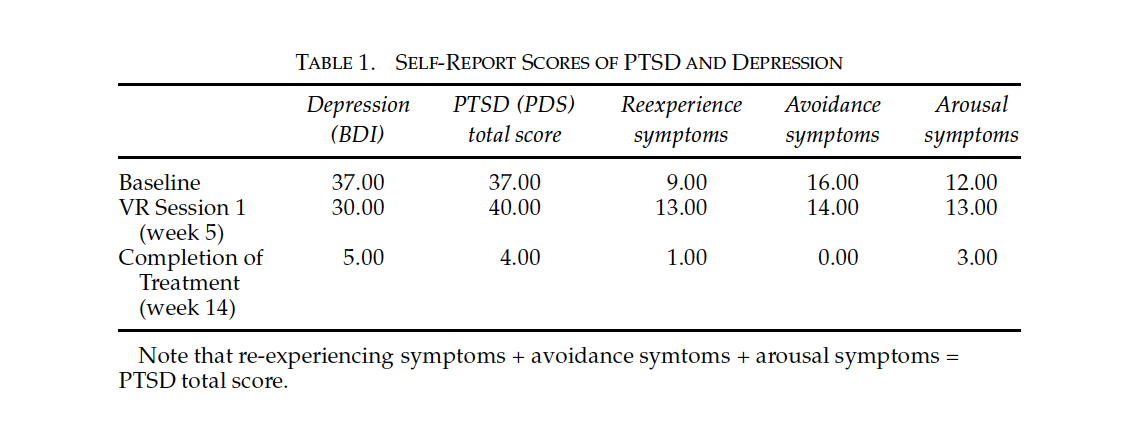
The study yielded the following results:
1. What conclusions can you draw from the results that are stated above?
2. What are the key limitations of using a case study of one patient to draw conclusions about the effectiveness of the treatment?
1. What conclusions can you draw from the results that are stated above?
We can conclude that the treatment was effective in significantly decreasing the symptoms of PTSD over the 14-week period. However, at the beginning of the treatment, there is actually a slight increase in the symptoms. This could potentially lead patients to drop out of the treatment as it could become more stressful for them. This is an important finding as this should be shared with patients when briefing them on the treatment strategy.
2. What are the key limitations of using a case study of one patient to draw conclusions about the effectiveness of the treatment?
The patient has certain characteristics that may influence how they respond to the therapy; for example, their age, level of education, gender, or culture. It is also difficult to carry out any valid statistical analysis of their progress as they may only be compared to themselves in a sample of one. In addition, the trauma experience and the treatment will be specific to the individual. That being said, in most mental health treatment studies, this is true regardless of the size of the sample.
Rizzo et al (2012) carried out a study of the effectiveness of VRET on 20 active-duty service members (mean age of 28). After eleven sessions, 16 of the 20 participants no longer met a diagnosis for PTSD and there was an average 50 percent decrease in symptoms among the remainder of the sample. In a follow-up to the study, the participants remained free of PTSD symptoms three months later. Self-reports from the participants suggested that they had seen an improvement in their quality of life.
Botella et al (2015) carried out a meta-analysis of studies on the effectiveness of VRET. One of the difficulties with assessing the therapy is that it is still relatively new. Originally, Botella et al found 439 studies of the effectiveness of VRET for the meta-analysis. When they eliminated all studies that were not in a peer-review journal, they were left with 124 studies. The majority of the studies were conducted on military personnel who had been sent to war zones. Although the meta-analysis indicated that VRET appears to be effective in the treatment of PTSD, there is the problem of a lack of controlled research to support that claim. More research is clearly necessary.
Individualized therapy can focus on the specific thinking patterns or concerns of the client. It is not a "generic treatment" like drug therapy. The client receives attention and support which results in a supportive relationship that is often absent in drug therapy.
VRET tends to have a low attrition rate - that is, few participants drop out of treatment.
- The therapy is still relatively new and there are not enough peer-reviewed studies that can be used to determine the effectiveness of the treatment
- There are some ethical concerns about any type of exposure therapy.
- Psychological treatments take a lot of time to start showing improvement. Although VRET shows results sooner than many other treatments, drug treatment may have to be applied in order for the client to successfully manage the VRET.
- Many studies are case studies - making it difficult to generalize findings or transfer the findings to other populations or forms of trauma.
- Most of the research on the effectiveness of VRET is carried out in Western cultures which tend to be individualistic. More research needs to be done to determine the extent of the cross-cultural application of the therapy.
Checking for understanding
Which of the following is not an assumption of Integrative Testimonial Therapy?
Why would Weine (1998) give the script of his conversations during therapy to the client at the end of the study?
Credibility is a term used in qualitative research to describe the validity of the interpretation of the researcher.
Which of the following is true of Integrative Testimonial Therapy?
Virtual Reality Exposure Therapy is based on the concept of
What is a limitation of research on the effectiveness of Virtual Reality Exposure therapy?
 Twitter
Twitter
 Facebook
Facebook
 LinkedIn
LinkedIn